











































Implementation of the World's Largest Measles-Rubella Mass Vaccination Campaign in Bangladesh: A Process Evaluation
International Centre for Diarrhoeal Disease Research, Bangladesh, or icddr,b (Sarma, Luies, Shamsuzzaman, Sultana, Ali, Uddin); the Australian National University (Sarma, Banwell); PATH (Budden, Rajaratnam); Institute for Health Metrics and Evaluation (Lim); Gavi, the Vaccine Alliance (Craw)
"The systematic identification of problems by all relevant stakeholders may contribute to a successful vaccination program."
The Expanded Program on Immunization (EPI) in Bangladesh, managed by the Ministry of Health and Family Welfare (MoHFW), conducted a national measles-rubella campaign (MRC) from January 25 to February 13 2014. Gavi, the Vaccine Alliance, funded the campaign, which included planning, training the health workforce, mobilising demand in communities, and procuring the MR vaccine. Gavi also supported a Full Country Evaluation (FCE) from 2013 to 2016, which demonstrated the MRC's reach (52 million children aged 9 months to 14 years) and effectiveness: MR vaccination coverage in a high-performing division increased from 4% before the MRC to 95% afterward and in a low-performing division from 11% to 85%. As part of the FCE, this group of researchers conducted a mixed-method process evaluation to understand the successes and challenges in implementation of the MRC.
The researchers implemented the process evaluation at the national, district, and community levels in both rural and urban areas of Bangladesh. They purposively selected 2 administrative divisions, out of 7 in the country, based on EPI coverage data: Rajshahi (high-performing), with 85.8% of children fully immunised, and Sylhet (low-performing), with 74.8% of children fully immunised.
After developing a theory of change to define milestones and indicators, the researchers: reviewed documents for the MRC and the immunisation programme in Bangladesh; observed meetings, vaccination sessions, and health facilities; and conducted 58 key informant interviews, 574 exit interviews with caregivers, and 156 brief surveys with stakeholders involved in immunisation.
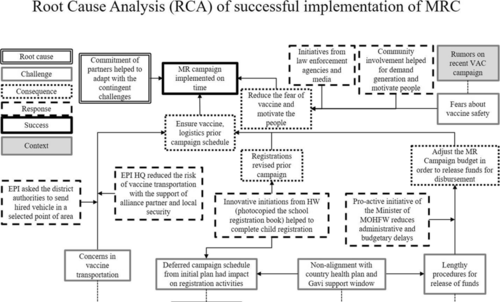
Figure 2 (see above) shows the results of root cause analysis on the implementation of the MRC. Initially, there were a number of challenges that delayed the implementation of the MRC - for example, concern about safe and on-schedule vaccine transportation, with the root cause being identified as political unrest. Despite these challenges, the MRC was found to have been implemented in a timely and successfully manner due to the commitment of partner organisations such as United Nations Children's Fund (UNICEF) and World Health Organization (WHO), which helped mitigate the challenges.
Multiple partner involvement was also key for developing an advocacy strategy and information, education, and communication (IEC) materials for the campaign. MoHFW promoted the campaign and worked to ensure full participation and support from all concerned authorities. The EPI developed IEC materials that were used from the national level to the community level. In addition, the EPI held advocacy meetings with Bangladesh Medical Association and the Pediatric Association to advise them of the MRC and to seek their support, including for disseminating information to parents. Furthermore, meetings were held with news editors from the press and electronic media to obtain their support for the publication of articles and messages to help create favourable public awareness and to counter instances of negative publicity, such as the false information that unknown sources circulated through short message service (SMS) to create panic regarding the poor quality of vaccines and the likelihood of causing adverse effects. These advocacy activities, conducted from the national to sub-national levels, "increased the community's awareness of the MRC and reduced the impact of negative propaganda around the MR vaccine."
Difficulties occurred around the timing of advocacy events, especially in hard-to-reach and remote areas. In response to these challenges, health workers used a variety of communication channels to disseminate messages. For example, a health worker with experience in hard-to-reach areas said: "We used mosques to make announcements regarding campaign activities in hard-to-reach areas, and if mosques were unavailable, we communicated with the community leaders in order to disseminate our information. Sometimes, we hired volunteers who lived in those areas to help us." As a result of such efforts, about 81% (95% confidence interval (CI) 77.6-84.0) of the mothers expressed satisfaction with the campaign, and about 78% (95% CI 74.3-81.1) reported that their children were vaccinated through the campaign.
In short, this evaluation identified challenges associated with the MRC relating to country-wide political unrest, administrative and budgetary delays, shortage of transportation, problems in registration of target populations, and fears about safety of the vaccine. Despite these issues, a number of elements contributed to the successful launch of the MRC: the comprehensive design of the campaign; strong partnerships between immunisation authorities in the government system, Alliance partners, and civil society actors; and motivated and skilled health workers at different levels of the health system.
In conclusion, the researchers "recommend that the EPI programme and its partner institutes work together to strengthen and sustain these partnerships for future vaccine introductions and to respond implementation challenges might occurred at different level of EPI programme, from national to community level. Lessons learnt from vaccine introduction campaigns of other countries are also of value in building capacity for EPI in low-income countries."
BMC Public Health 2019 19:925. https://doi.org/10.1186/s12889-019-7176-4
- Log in to post comments