











































Silent Reintroduction of Wild-type Poliovirus to Israel, 2013 - Risk Communication Challenges in an Argumentative Atmosphere
Public Health Services, Ministry of Health (Kaliner, Moran-Gilad, Grotto, Kopel); Faculty for Health Sciences, Ben-Gurion University of the Negev (Moran-Gilad, Grotto, Gdalevich); Paediatric Infectious Diseases, Wolfson Medical Center (Somekh); Sackler Faculty of Medicine, Tel-Aviv University (Somekh, Gamzu); South District Health Office, Ministry of Health (Gdalevich); Ministry of Health (Shimron, Amikam, Leventhal, Lev, Gamzu)
"Lessons learned from our recent experience may inform risk communication approaches in other countries that may face a similar situation as global polio eradication moves towards the 'End game'."
This paper reviews the challenges faced by Israel's Ministry of Health (MoH) and the communication strategy devised in order to facilitate and optimise the various components of the public health response to a risk communication situation involving polio vaccination. Certified as polio-free by the World Health Organization (WHO), Israel's routine immunisation (RI) schedule consists of inactivated poliovirus vaccine (IPV) only. Yet, at the end of May 2013, the MOH confirmed the reintroduction of wild-type poliovirus (WPV) 1 into the country. Documented ongoing human-to-human transmission necessitated a thorough risk assessment followed by a supplemental immunisation campaign using oral polio vaccine (OPV). "The unusual situation in which ongoing poliovirus transmission was picked up through an early warning system of sewage monitoring without active polio cases, brought about significant challenges in risk communication..."
On August 5 2013, the MoH decided to conduct a supplemental immunisation activity (SIA) to vaccinate all children aged from 0 to 9 years in the southern region of the country who had not received OPV in the past, with a bivalent oral polio vaccine (bOPV). Two weeks later, following continuous circulation of WPV1, the SIA was extended to cover the entire country. By mid-October, more than 900,000 children of 1.2 million candidates were vaccinated. Seemingly, this coverage rate had a favourable epidemiological effect - as judged by the dramatic reduction in prevalence of WPV1 detected during environmental surveillance and field surveys - "but was it successful from a risk communication point of view? How can health authorities improve compliance during SIAs?"
The MoH's communication and media experts, as members of the national outbreak control team, developed a communication strategy during the early phase of the process that focused on the basic principles of trust, early announcement, transparency, "the public", and planning. In accordance with this approach, within one day after the confirmation of WPV1 circulation in the country, a report using information available to the MoH was made public. The rationale underlying early announcement was to provide information to the media and establish the MoH as the most reliable source while aiming at preventing media reports of rumours and speculations, especially via social media. Similarly, the media and the public were informed about any new data generated from environmental surveillance and population surveys and about subsequent public health response, in a timely manner (e.g., official media briefings). To prevent a situation where the public receives information before healthcare professionals, a major effort was undertaken to ensure that all briefing materials intended for both professionals and lay public were prepared simultaneously and distributed first to healthcare professionals and MOH employees and immediately afterwards to the public.
There was also a planned communication strategy in preparation for the SIA. Following consultations with WHO experts during their mission to Israel, a decision was made to design two campaigns: one that would focus on hygiene and be launched before starting the SIA and another one that would focus on vaccination. As a complementary measure, the MoH sought counselling from a commercial strategic consulting firm to prepare the communication plan and to design key messages for the public. Moreover, the firm was asked to advise on management and monitoring of communication in electronic media - in particular, social networks that were identified during the 2009 influenza A(H1N1) pandemic. In the planning process, organisers identified 3 potentially critical communication points:
- There was a need to achieve consensus amongst the medical community regarding the need for a SIA. Discussions and briefings of chairs of national medical societies, national medical councils and the Israeli Medical Association, as well as information delivery to the entire medical community were activities carried out to engage paediatricians, family physicians, and infectious disease and neurology consultants. Points of contact at the MoH Public Health Services were established to provide feedback and consultation to frontline physicians. In weeks after the decision to deploy the SIA, dozens of conferences were held by MoH senior representatives in every hospital in the country and in every region. At the political level, the Israeli Government received periodic briefings, and the Health Minister was engaged in key decisions. An example of engagement: Paediatricians' attitudes were monitored by their inputs into the paediatric professional electronic network (IPRONET) that is used by 500 paediatricians across Israel. IPRONET communications and small focus groups held prior to the campaign revealed that most paediatricians declared that they were neither going to recommend OPV to their patients nor vaccinate their own children, due to the perceived low risk-benefit ratio of OPV. This was mitigated by 7 informal information papers and daily responses to frequently asked questions (FAQ) by senior paediatricians in their network during the SIA together with direct formal email briefings from the MoH regarding the status of WPV1 circulation and rationale for the SIA, using email contact lists provided by medical organisations and associations.
- Anticipating that anti-vaccination groups would take advantage of the situation and attack vaccines in general and the "new" polio vaccination with bOPV in particular, it was decided not to confront those movements head on, but, rather, to prevent them from negatively influencing the general public.
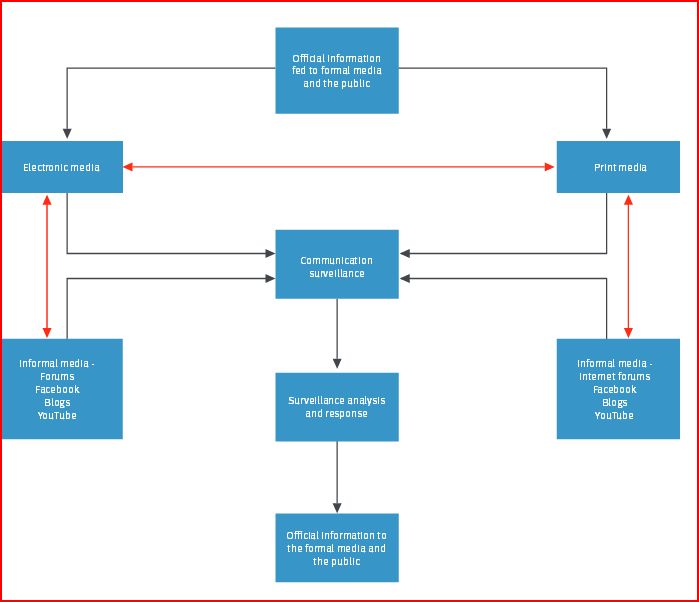
- The rationale for the SIA using OPV was complicated to deliver; it was even harder to motivate the public to take action and get vaccinated. "Many parents felt that OPV was a 'social' vaccine that builds on herd immunity and compensates for the small percentage of the population that has not received IPV, and felt that administering OPV to their IPV-vaccinated children is merely altruistic. Mindful of that, the message to the public was that the vaccine will protect their family members and close friends and not just the individual or the 'environment' or 'society'." Examples of communication channels used by the MoH in the incident under discussion included: (i) a new designated official polio MoH website, (ii) an existing official Facebook interface, (iii) an existing national call centre involving over 20 MoH staff for several weeks reinforcing polio communications (agreed key messages and answering FAQ), (iv) print media (national and sectorial in various languages), and (v) electronic journalism, including various social networks, forums, and blogs. Information was provided in all common languages spoken in Israel.
In terms of communication strategy during the SIA itself, the MoH decided on a massive and continuous presence of public health professionals who had undergone ad hoc training to answer questions, eliminate ambiguity, and rectify disinformation through online and traditional media. "One of the problems that arose from deployment of multiple responders, however, was occasional lack of uniformity in messages. Rare cases of contradicting messages (almost always concerning minor issues) were picked up by vaccination opponents and used for attacking the campaign and questioning the MoH credibility. Frequent briefing of professional responders aimed at preventing such situations, but uniform messaging remains a challenge for management of future incidents. By the time the SIA was launched, the continuous sharing of information and transparency had harnessed almost all health journalists to support the SIA and its objectives."
In addition, during the campaign, public figures were recruited to support it, including members of the Knesset, the Israeli parliament, and the president of Israel. MoH physicians were photographed while vaccinating their family members as reassurance to inquiries from members of the public who questioned whether health professionals practise what they preach. At the individual level, phone calls and SMS (text) messages to parents who did not vaccinate their children were used to provide information as needed. Monitoring of the media was performed throughout the SIA in order to identify "hot" issues. For example, one of the arguments of the vaccine opponents was that the MoH had yielded to international pressure from WHO and other international health authorities as part of a global campaign and not a local need. The risk perception of the vaccine was enhanced and public anxiety was directed towards vaccine associated paralytic polio (VAPP) rather than the risk from WPV1 circulation. In order of mitigate those concerns, data from post marketing safety surveillance, the package insert of the vaccine, laboratory testing results of the specific bOPV lots used, and clinical trials done with the vaccine were published on the official MoH website and questions in social media answered by a dedicated MoH specialist.
The report offers specific lessons learned from this polio communication strategy. In brief:
- "[H]ealth authorities need to assess their methods of communication before and during an outbreak of infectious disease. This is certainly true in a major event that lacks concurrent morbidity. Risk communication in relation to vaccine-preventable diseases (VPDs) involves certain unique aspects, especially those related to the safety, efficacy and effectiveness of vaccination, and social factors such as anti-vaccination movements, conspiracy theories and ethical discourse surrounding equality, autonomy and mutual guarantee."
- While the importance of the internet as key media was acknowledged and emphasised in this campaign, billboards, radio, television, and traditional mail messages proved particularly useful among specific sectors with limited internet use.
- Reliable information on vaccines should preferably be made available routinely and not only when an SIA is contemplated. It is suggested here that pro-vaccine websites include narratives and stories of patients or family members thereof who fell ill with VPDs. "It is important to work on the image of the health authority as a credible source of information and judicious decision maker, throughout the year, so that the level of trust in the information provided will be high during public health emergencies."
- Efforts were made to strengthen health communication interventions through the adoption of a more holistic ecological model of people and their health-related behaviours - analysed in the context of larger social, economic, political, and cultural forces. For instance, Israel is characterised by a heterogeneous population, consisting of social, ethnic, or religious communities with distinctive cultural characteristics. For each group, messages were delivered taking into account cultural and linguistic barriers as well as direct approach to ensure engagement of community leaders.
The report concludes by offering reflections and several unanswered questions, such as: Is it appropriate to involve non-professionals in a decision making process that is fundamentally professional? Will inclusion of antivaccinist group representatives in the process soften their opposition or just feed information that could be used against vaccination? Can there be too much information in public health messaging? With regard to the latter question, further questions emerge: "Interestingly, the links to anti-vaccine sites in the Internet still appear higher up than the MoH official site in Google searches when typing the word 'polio'. This is exemplified by antivaccinist and MoH 'YouTube' movies ranking 1st and 10th in Hebrew Google search of 'polio', respectively, despite the fact that the MoH movie has gained over 200,000 views as compared to only 25,000 for the anti-vaccine movie. Overall, this emphasises the continuous challenge health authorities are facing, even when risk communication is planned thoroughly and performed systematically."
Eurosurveillance, Volume 19, Issue 7, February 20 2014.
- Log in to post comments