











































Why Is Announcement Training More Effective than Conversation Training for Introducing HPV Vaccination? A Theory-Based Investigation
University of North Carolina
Evidence shows that a strong provider recommendation can substantially increase human papillomavirus (HPV) vaccine acceptance, but that many recommendations in the United States (US) are of low quality or absent. This group of researchers previously demonstrated that training providers to use a presumptive approach ("announcements" like "Your child is due for this vaccine") to introduce HPV vaccination improved uptake, whereas training them to use participatory conversations (e.g., "What questions do you have about this vaccine?") had no effect. To understand how communication training changed provider perceptions and communication practices, in the present paper, they evaluate intermediate outcomes and process measures from the earlier randomised clinical trial, with a particular focus on identifying mechanisms that might explain the announcement training's impact.
The researchers conducted the randomised clinical trial of 30 primary care clinics in North Carolina to assess the impact of announcement and conversation communication training on HPV vaccination coverage. They developed the trainings based in part on the theory of planned behaviour (TPB), which posits that one's attitude toward a behaviour, perceptions of subjective norms about a behaviour, and beliefs about one's capability of performing a behaviour and its impact (i.e., perceived behavioural control) increase intentions to act (e.g., intentions to recommend HPV vaccine), which, in turn, leads to the behaviour (e.g., HPV vaccine recommendation). From May to August 2015, a physician educator delivered the 1-hour trainings to vaccine-prescribing clinicians and other staff at intervention clinics. Trainees included 83 vaccine-prescribing and 59 non-vaccine prescribing clinicians practicing at 20 clinics serving 11,578 adolescents ages 11 or 12 and 24,069 adolescents ages 13 through 17.
Among 11- to 12-year-old patients, the researchers found that training providers to make presumptive announcements about HPV vaccine increased coverage by 5%, whereas training providers to start participatory conversations did not result in statistically significant improvements in coverage.
It was found that providers shifted their communication style to match the style in the training they attended. Before the training, providers reported using conversations more often than announcements (mean [M] = 3.5 vs. 2.5, p <.001, Cohen's d = .68), a finding that did not differ by trial arm. A month later, providers who received the announcement training reported a higher frequency of using announcements compared to providers in the conversation training (M = 4.0 vs. 3.3, p = .01, d = .58). Similarly, providers who received the conversation training reported a higher frequency of using conversations at 1-month follow-up compared to providers who received the announcement training (M = 3.7 vs. 3.2, p = .03, d = .49). For use of conversations, the interaction between time and trial arm was statistically significant (p = .03) due to rising use of conversations in the conversation training arm and falling use in the other arm.
Quality of recommendation practices increased as well for both trial arms combined. The recommendation quality index increased from an average of 4.9 (standard deviation [SD] = 1.2, range 0–6) at pre-training to 5.3 (SD = 0.7, range 2–6) at 1-month follow-up (p = .001, d = .36). Emphasis on cancer prevention in discussions and recommendation consistency did not change. While trial arms did not differ on recommendation quality measures by 1-month follow-up (all p>.05), change in recommendation quality differed for the 2 trial arms (p
The amount of time providers said they spent discussing HPV vaccine decreased from pre-training to 1-month follow-up (M = 3.8 vs. 3.2 min, p = .01, d = .28). Providers in the announcement arm, compared to the conversation arm, had higher perceptions at 1-month follow-up that using the strategy saved them time (p = .01, d = .58).
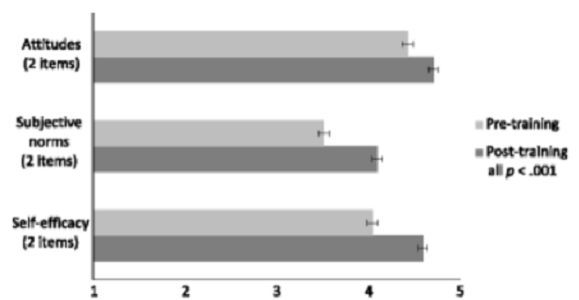
Providers had increases in positive attitudes toward HPV vaccination from pre- to post-training (M = 4.4 vs. 4.7, p <.001, d = .62). They also had increases in subjective norms (M = 3.5 vs. 4.1, p <.001, d = .90) and perceived behavioural control to recommend the vaccine (M = 4.1 vs. 4.6, p <.001, d = .89). At 1-month follow-up, providers who received announcement training, compared to conversation training, reported greater levels of agreement that they felt confident addressing parents' concerns when discussing HPV vaccine (M = 4.8 vs. 4.4, p <.01, d = .73).
Announcement training, compared to conversation training, elicited more favourable post-training perceptions that using the strategy would be easy to do (p = .02, d = .52), help them promote HPV vaccination as part of routine adolescent care (p = .04, d = .44), help them address parents' HPV vaccine concerns (p <.01, d = .63), and help them emphasise HPV vaccine as a way to prevent cancer (p = .02, d = .47). The researchers speculate that "providers perceived announcements as being more feasible and therefore implemented that strategy more often. It may be that providers' positive perceptions of the announcement training, along with TPB-related constructs, were needed to drive the higher HPV vaccine coverage...observed in announcement training clinics."
The researchers reflect: "Given that providers have little extra time, it is encouraging that a brief continuing medical education activity could make them more efficient while also increasing recommendation quality....Providers reported making recommendations that were timelier, stronger, more urgent, and routine after the training, but in two areas quality did not increase. Communicating HPV vaccination as cancer prevention did not increase, perhaps because it was already so common. However, the lack of change in providers' consistency of HPV vaccine recommendation - i.e., recommending vaccine for all children regardless of perceived HPV risk—represents a concerning divergence from national recommendations for routine HPV vaccine delivery....[This] finding highlights the need for further research on ways to improve this aspect of provider communication. Modifying the training to include a stronger emphasis on the importance of and rationale for routine HPV vaccination may improve providers' recommendation consistency."
Future studies could be carried out to:
- Understand how communication training affects the experience of adolescent patients and their parents; like providers, families may appreciate spending less time on routine preventive services so as to focus on more complex health issues.
- Collect survey outcomes and process data from providers in the control arm so as to offer additional insight into how the trainings acted on the TPB constructs.
- Consider implementation outcomes, including acceptability, alongside more traditional TPB constructs.
Implementation Science 2018 13:57. https://doi.org/10.1186/s13012-018-0743-8
- Log in to post comments