











































Implementing People-centred Health Systems Governance in 3 Provinces and 11 Districts of Afghanistan: A Case Study
Management Sciences for Health, or MSH (Anwari, Shukla, Boyd-Boffa, Trasi); Wardak Provincial Public Health Office (Maseed, Wardak); Khost Provincial Public Health Office (Sardar); Herat Provincial Public Health Office (Matin, Rashed); Ministry of Public Health (Hamedi, Sahak, Aziz)
"WHO calls a health system people-centred when it is rooted in principles of human rights and dignity, nondiscrimination, participation and empowerment, universal access and equity, and partnership..."
Fragile contexts, which are characterised by a cycle of insecurity, deficiencies in the delivery of public services, and mistrust, face particular challenges when it comes to governing well. Studies have demonstrated that good governance, especially at decentralised levels, can improve health outcomes. This paper presents the results of a year-long intervention that placed a people-centred health systems governance approach in the hands of multi-stakeholder committees in 3 provinces and 11 districts in Afghanistan.
As defined here, governance is good when: (i) decisions are based on information, evidence, and shared values; (ii) the process is transparent, inclusive, and responsive to the needs of the people, the ministry, or the organisation it serves; (iii) those who make and those who implement decisions are accountable; (iv) strategic objectives are effectively, efficiently, ethically, and equitably met; and (v) the vitality of the organisation and the services it provides are sustained.
The governance structure in Afghanistan involves, at the central level, non-government organisations (NGOs) that the Ministry of Public Health (MOPH) has contracted to provide services through health posts and health facilities. Meanwhile, Provincial Public Health Coordination Committees (PPHCCs) are formal multi-stakeholder committees established by the MOPH at provincial level that provide a forum for coordination and information sharing among various stakeholders in the provincial health system. District Health Coordination Committees (DHCCs) perform a role similar to that of the PPHCCs in the provinces.
The pilot was conducted in 4 phases:
- Provincial and district health systems governance guides were drafted, based on effective governing practices, in consultation and with participation of PPHCCs and DHCCs.
- Based on the guides, 3 PPHCC and 11 DHCC teams participated in four 2-day workshops facilitated by public health and governance experts, where they designed a specific governance development action plan. (Examples of planned activities for improving stakeholder engagement would be: interviewing patients and health service users; inviting religious, youth, and women leaders to meetings; providing feedback to consultative assemblies at health facility level; and/or consulting community leaders on a regular basis.) They also measured their governance at baseline using 5 self-assessment instruments.
- The committees implemented and monitored their action plans over a period of 6 months.
- The committees evaluated their implementation of the action plans and measured their governance post-intervention (6 months later) using the same 5 self-assessment instruments.
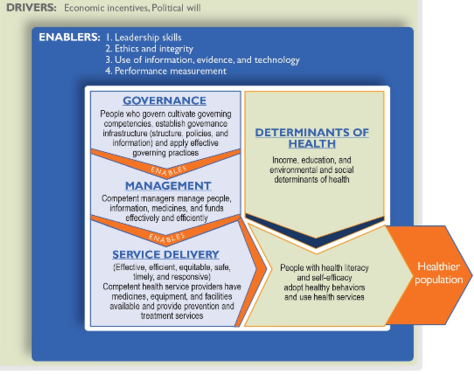
The paper documents the application of this people-centred health systems governance conceptual model based on applying 4 effective governing practices: cultivating accountability, engaging with stakeholders, setting a shared strategic direction, and stewarding resources responsibly. The fifth practice of periodically assessing governance and continuously trying to enhance it ensures that the 4 practices are consistently applied. On the participatory approach based on these practices and depicted in the conceptual model, above, health system leaders identify and act on opportunities for making themselves and their health systems more accountable and responsive to the needs of the communities they serve.
The mixed-methods exploratory case study uses analysis of governance self-assessment scores, health management information system (HMIS) data on health system performance, and focus group discussions. The outcomes of interest are governance scores and health system performance indicators.
Project implementers expected to see change in maternal and child health indicators because maternal and newborn care, and child health and immunisation, are the top 2 of the 7 elements of the Basic Package of Health Services, and this package is the mainstay of the primary health care in Afghanistan. The evaluation did not find a statistically significant impact of the intervention on health system performance or health outcomes, except that antenatal care visit rate in the pilot provinces increased by 20%.
The pilot PPHCCs and DHCCs reported a high level of completion of their governance development action plans, and committees planned to continue 76-98% of these actions in the future. In addition, PPHCC and DHCC self-assessment of governance performance at baseline and again after 6 months of pilot testing indicated that PPHCCs improved their governance score on average by 13.2% and 18.5% using 2 different scales (one based on roles and responsibilities and the other on governance standards), and individual PPHCC members improved their governance score on average by 6.7% and 9.7%, also using 2 different scales (one based on governing practices and the other on governance competencies). DHCCs improved their governance by more than 20%. Improvement was higher in the provinces and districts where leaders were more committed to a people-centred approach, as inferred from the extent of completion of their governance development action plans.
Eleven focus group discussions indicated improvements across the 4 governing practices, including, for example:
- Enhancing transparency and accountability - The PPHCC and DHCC members reported that: Their activities as a committee became more transparent and involved diverse stakeholders; intersectoral coordination and collaboration improved; there was an improved focus on patients' health problems at the community level; community health needs were defined and discussed; coordination, communication, and information sharing improved; the frequency of data analysis and presentation to the committees increased; and more committee decisions were evidence based.
- Including stakeholders and stakeholder views - The members reported that: Steps were taken to recruit more women to community health nursing educator posts; suggestion and complaint boxes were placed outside health posts, and the community complaints were discussed during regular meetings; attendance of members at the meetings improved; civil society groups, community leaders, and representatives from other sectoral departments were invited to the committee meetings; community concerns were discussed as a standing agenda item during committee meetings; and vaccination rejection in some villages was addressed by negotiating with elders and through community mobilisation efforts.
- Setting a shared strategic direction - The members reported that: The MOPH guidelines and policies were introduced and shared in the PPHCC and DHCC meetings; service delivery data was analysed and shared more frequently with committee members; and annual plans were developed and shared with the stakeholders in the province and the MOPH.
- Stewarding resources responsibly - The members observed that there was a better link between committees at provincial and district levels. Communities began participating in health facility monitoring, gave feedback on the quality of health services, and became motivated to contribute to health service delivery improvements.
Overall, committees reported notable changes in their knowledge, skills, and behaviours, including feeling more capable, responsive, and accountable than they were before the intervention. Committee functioning became more systematic and regular, and members felt more responsible for their decisions. Committees also noticed improvements in their effectiveness; referral of TB cases for treatment improved in one district, un-served remote areas were identified, and 90% of them were covered through establishment of mobile teams in another district. Because of increased community engagement, committees felt they could solve problems at the health facility level in collaboration with the local community. This experience showed them that they could build trust with the communities by working with them.
Lack of resources emerged as one of the most common challenges the committees faced in completing their action plans. The security situation often prevented engagement of provincial and district governors, and also did not allow for the level of health facility monitoring that the committees would have liked to achieve. Resources for training and education of committee members were found to be inadequate.
Lessons learned, in brief:
- A framework of effective governing practices makes governance enhancement accessible to the leaders.
- Participation of the governance leaders enhances their commitment.
- Placing people at the centre of the intervention brought life to it.
- Governing bodies at decentralised levels can represent community concerns and resolve them.
- Governance improvements need time to translate into improved health system performance.
- Leadership of the ministry matters.
In conclusion, this study "provides a potentially useful approach to improving governance of health systems in a fragile and conflict affected environment. These study results may be applicable to similar settings where governing bodies or committees governing provincial or district health systems wish to adopt people-centred health systems governance approaches. Future studies should consider longer duration and more rigorous research design that test whether improved health systems governance leads to higher health system performance and improved health outcomes."
Conflict and Health 2015,9:2. http://www.conflictandhealth.com/content/9/1/2
- Log in to post comments