











































Designing for Impact and Institutionalization: Applying Systems Thinking to Sustainable Postpartum Family Planning Approaches for First-Time Mothers in Bangladesh
Save the Children US (Yahner, Mangieri); independent consultant; formerly of Save the Children Kenya (Muriuki); Save the Children Bangladesh (Nitu); independent consultant; formerly of Save the Children Bangladesh (Shafinaz); Gavi, the Vaccine Alliance; formerly of Save the Children US (Sarriot)
"...experience shows that considerations of sustainability can be feasibly incorporated into design processes."
In many low- and middle-income countries (LMICs), multiple family-, community-, and health system–level factors shape first-time mothers (FTMs)' postpartum family planning (PPFP) use. Thus, most efforts seeking to reach FTMs have entailed multilevel approaches coupling integrated service delivery, including fostering respectful care, with community-level interpersonal communication efforts to address normative and social factors that limit service use. Such complex, multilevel FTM initiatives have proven challenging to fully scale and institutionalise. Drawing on Connect project (2019-2024) approaches to increase PPFP use among FTMs in Bangladesh, this paper outlines a practical method for designing integration approaches with potential for both impact and institutionalisation.
Led by Save the Children with funding from the Bill & Melinda Gates Foundation, the Connect project aims to develop sustainable PPFP approaches for FTMs in Bangladesh and Tanzania; the present article focuses on the work done in Bangladesh. In 2020, the project design team formulated scalable PPFP integration approaches that showed (i) potential for impact with the priority population, based on global evidence and formative research; and (ii) potential for institutionalisation, based on organisational management conditions of the health system. The team adapted a management systems theory, the Viable System Model (VSM), which presents 5 essential organisational functions and the relations required between them to improve the viability (performance and institutionalisation) of organisational systems.
The paper outlines each step in the process, which included:
Formative phase: The team led a formative barrier and facilitator analysis in 2 upazilas of Noakhali district in Chattogram division, using participatory qualitative methods to identify factors influencing FTMs' use and nonuse, and delayed initiation and discontinuation, of reproductive, maternal, newborn, and child health (RMNCH) services including PPFP, as well as to identify factors influencing health system responses to FTMs' needs. The analysis used a socioecological approach, sampling 20 FTMs, 10 male partners, 4 facility-based providers, and 14 community-based providers. The team synthesised findings, pinpointing the key barriers to PPFP use that the approach would need to address. In short, the analysis found that mothers-in-law and male partners determined whether and where FTMs accessed RMNCH services; FTMs had limited negotiation power within family structures. Many PPFP adopters discontinued method use within 12 months due to side effects and pressure to become pregnant again. Mothers of all ages had increased responsibilities and restrictions on movement outside the home for 40 days postpartum due to religious and social prohibitions, which limited facility visits. During this formative phase, the team also identified considerations for potential institutionalisation.
Design phase:
- For each of 8 modules, a core design team engaged stakeholders through synchronous video meeting components interspersed with asynchronous work (e.g., background reading, follow-up emails, and smaller group discussions). As part of this process, the team gathered ideas and organised by the entry point at which FTMs would be reached for the first time (i.e., during antenatal care [ANC] [6 ideas], during intrapartum or predischarge care for those delivering in facilities [4 ideas], through immunisation services [4 ideas], through special care for small and sick newborns [2 ideas], or at the community level [4 ideas]). The team then prioritised 1 idea from each entry point for further discussion. For each of these 5 ideas, the team developed a visual client journey map. To operationalise the VSM to the questions faced by primary healthcare systems in Bangladesh in integrating PPFP into existing services, the core global project design team developed the Viability Assessment Tool (VAT) through an iterative process over Modules 4-7. The VAT used a client-centred approach following an FTM's journey through the Bangladesh primary healthcare system. Bangladesh-based members of the core design team defined intervention packages (e.g., tools, trainings) and considered the implications of each of the 5 short-listed approaches. They found that some initially promising approaches (i.e., PPFP/immunisation integration) required system shifts infeasible to institutionalise or scale.
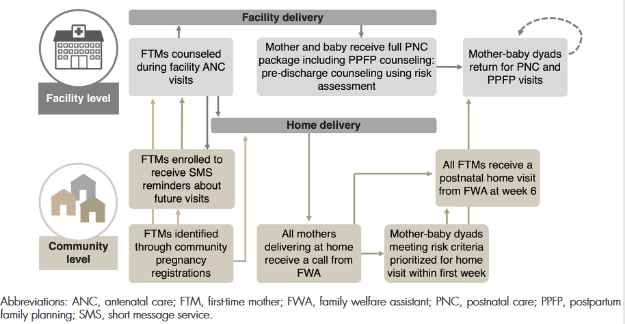
- Ultimately, the core design team selected 3 of the approaches (strengthening immediate PPFP, strengthening predischarge counselling, and supporting postnatal home visits, or HVs) to be combined into a final approach, which aims to increase uptake of PPFP through strengthening the quality and responsiveness of facility-based antenatal and postnatal counseling and care (including predischarge counselling and care) to FTMs. At the community level, family welfare assistants (FWAs) are supported to provide targeted postnatal HVs, during which they distribute a mother-baby booklet written for girls and young women becoming FTMs and their male partners, as well as a printed invitation card that invites FTMs to access RMNCH services, including PPFP, from the closest health facility.
Reflecting on the experience, the team notes that the application of the VSM provided structure to guide stakeholders to identify the strengths and limitations of the platforms under consideration. Close engagement with national stakeholders, as system experts and owners of institutionalisation and scale, was also key. Other lessons learned:
- Combined, the selected approaches align with existing job descriptions and supervision processes, with mitigation measures to address identified gaps in workload, information, documentation, and supervision. Furthermore, the targeted approach to HVs is essential to reaching FTMs regardless of place of delivery and to engaging family.
- Contextual factors, including health system structure and capacity, are important to consider in developing and adapting interventions and planning for sustainability.
- Further exploration of a systems-thinking-informed means to identify and articulate displacement risks (e.g., saturating the capacity of existing human resources, such as increased workload or shifted client flow, or displacing priorities to the detriment of other essential services) beyond the intervention design phase is warranted.
In conclusion: "Considerations of the feasibility of institutionalizing impactful approaches are underemphasized and require deeper attention in global health efforts, to the same level as the focus on the potential for an approach to produce desired impacts. Any approach has risks to sustainability; considering organizational functions in the design process can inform proactive mitigation approaches and ongoing monitoring efforts."
Global Health: Science and Practice October 2022, https://doi.org/10.9745/GHSP-D-22-00023
- Log in to post comments